There is no information in the literature on the ratio of the concentrations of Endocan, PAI-1, and intima media thickness (IMT) in patients with high diabetes risk. This study aims to investigate the relationships between endothelial dysfunction biomarkers: Endocan, Plasminogen Activator Inhibitor-1(PAI-1), insulin resistance (IR) indicators, and IMT of the common carotid artery (CCA) in patients with risk of type 2 diabetes mellitus (T2DM). A case-control study was held, including 184 individuals, aged from 18 to 65 years. According to FINDRISC scale, patients were divided into 2 groups: Group 1 (n = 138) — low risk of T2DM (<12 points) and Group 2 (n = 46) high risk of T2DM (>12 points). IMT more than 0.9 mm on ultrasound considered as an atherosclerosis. Significant differences were found when studying the level of Endocan, PAI-1 biomarkers with their predominance in the group of patients with a high risk of T2DM; concentrations of Endocan comprised (mean±SD) 1698.2±576.2 pg/ml; p=0.01; PAI-1–32307.15±19947.12 pg/ml; p=0.05 to compare with low risk of T2DM. In addition to, mean values of IMT prevailed in patients in the group with a high diabetes risk and comprised right IMT CCA-0.90±0.15 mm; p = 0.05, left IMT CCA- 0.91±0.14 mm; p=0.02. Interrelations between Endocan, PAI-1, and IMT CCA have been determined by correlation analysis. These findings indicate that in patients with high diabetes risk the elevations of the Endocan, PAI-1 is associated with a subclinical atherosclerosis. Furthermore, both biomarkers Endocan and PAI-1 has been demonstrating significant correlation with insulin, IR-HOMA index, С-peptide, HbA1c, and fasting glucose in patients with high risk of T2DM. We found significant relationships between the ED biomarkers with IMT and IR in patients with high risk of T2DM. We suggest that rising of IR leads to Endocan and PAI-1 elevation, subclinical atherosclerosis and thereby increase ED and cardiovascular risk in these patients.
Introduction
Type 2 diabetes mellitus (T2DM) is one of numerous risk factors for the development of cardiovascular events (CVE), leading to the progress of endothelial dysfunction (ED), and subsequently to mortality from macrovascular complications [1]. CVE assassinates millions of people every year, and cardiovascular diseases (CVD) still occupy a leading position worldwide in terms of morbidity and mortality from noncommunicable diseases. According to the WHO, in 2016, 17.9 million people died from cardiovascular diseases, 31 % of all deaths in the world [2]. In Kazakhstan, this indicator was also at a high level and amounted to 25.9 % [3].
Insulin resistance (IR) is the main pathogenetic link of prediabetes and T2DM, contributes to the development of hyperinsulinemia, leading to endothelial dysfunction (ED) followed by an increase in blood pressure (BP), progression of atherosclerotic vascular changes, impaired hemostasis. The issue of in T2DM has been studied in numerous studies. Complex intersections of the metabolic pathways of insulin resistance (IR) and ED simultaneously affect the atherosclerosis, with no possibility to say exactly which of these processes increasingly damages a vessel wall. At the same time, hyperglycemia in DM induces the endothelial dysfunction through oxidative stress, and also contributes to the accelerated atherosclerosis [4, 5]. Thus, the ED and vascular disorders result in macroangiopathy and CVE in T2DM patients.
CVE in patients with prediabetes are not well understood since prediabetes itself is a poorly diagnosed condition, and, accordingly, CVE due to the presence of prediabetes are also little understood. It was found that an increase in the level of glycated hemoglobin of more than 6 % is associated with development not only of diabetes, but also of CVE [6].
To assess the risk of T2DM, FINDRISC scale was chosen [5]. This scale estimates the 10-year risk of T2DM, including asymptomatic diabetes and impaired glucose tolerance (IGT), with 85 % accuracy. This scale is validated, adapted to our population (considering the nature of diet, physical activity), low-cost and easy to use.
There are several studies on cardiovascular risk (CVR) in patients with a high risk of diabetes on the FINDRISC scale [6–8], it was established high diabetes risk was associated with not only impaired insulin secretion and insulin sensitivity, but also with high cardiovascular risk. This is also consistent with the results of our previous study on CVR in patients at high risk of T2DM [9]. Results have demonstrated that patients with the high diabetes risk contemporaneously have the high cardiovascular risk on the SCORE scale.
There is only one study examining IMT in patients with T2DM risk. The results of study [10] show that patients with a high risk of T2DM and prediabetes have all ultrasound signs of subclinical atherosclerosis. However, no studies have been conducted to assess the ratio of the levels of the Endocan, PAI-1 (plasminogen activator inhibitor), and IMT, and effect of biomarkers on the IMT in patients with T2DM risk.
In our present study, we pursued the goal of assessing subclinical atherosclerosis by studying the intima media thickness (IMT), which is a sensitive indicator of the risk of CVE.
Thus, the scientific novelty and research issue of our study is the assessment of endothelial function by measuring the IMT in conjunction with the measurement of the Endocan, PAI-1 biomarkers concentrations in patients with T2DM risk, as well as the effect of IR on ED, as a result the development of subclinical atherosclerosis in these patients.
The paper aims to study the association of IR, Endocan and PAI-1 biomarkers and the IMT in patients with risk of T2DM.
Experimental
The unmatched case-control study was carried out among the population of Karaganda city, Kazakhstan, from January 2019 to December 2019, in polyclinic of the city. The study involved 184 respondents. There were 73 (39.6 %) males and 111 (60.4 %) females.
The respondents were divided into 2 groups:
Group 1 “case” — respondents with a high risk of T2DM on the FINDRISC scale n = 46 (25.0 %);
Group 2 — “control” respondents with a low risk of T2DM was, n = 138 (75.0 %) [5].
Sample size.
Sample size was calculated using the Kelsey method, EPI info software for case-control studies without matching. The two-sided confidence level was 95 %, the statistical power was 80 %; the ratio of unexposed cases to exposed cases was two. According to literature review, we took data about prevalence patients with T2DM from previous studies. Thus, after calculation the minimum number of respondents with a high diabetes risk was 46 people (case), patients without or low diabetes risk (control) — 92 people.
Assessment risk of T2DM on the FINDRISC scale.
The risk of T2DM was assessed using the FINDRISC scale, the questions of which included information on age, BMI, WC, having at least 30 minutes of physical activity daily, taking antihypertensive drugs, data on the presence of diabetes in relatives, data about previously increased blood glucose levels, daily consumption of fresh vegetables [5]. This scale allows determining the ten-year risk of developing T2DM with 85 % accuracy. All respondents were divided into 2 groups: low and high risk of T2DM. The group of low risk T2DM included respondents with number of points less than 12, and the group of high risk T2DM — included respondents with number of points more than 12 on the FINDRISС scale.
Respondents:
Inclusion criteria:
Males and females aged from 18 to 65 years, without a previously diagnosis of T2DM, after filling out their informed consent.
Exclusion criteria:
- Patients with a previously diagnosed T2DM or newly diagnosed diabetes by an oral glucose tolerance test, or patients with random plasma glucose level of 11.1 mmol / L (200 mg / dL) or higher were excluded from the study.
- Patients with a previous history of acute and decompensated heart disease, including myocardial infarction, cerebral stroke, confirmed by coronary angiography and CT were excluded from the study.
- Patients with chronic kidney disease and renal dysfunction based on a glomerular filtration rate (GFR / CKD-EPI) less than or equal to 90 ml / min / 1.73 m2 were excluded from the study.
Pregnant women, people with severe mental and oncological diseases also were excluded from the study.
Before starting the study, all respondents completed their informed consent.
Ethical approval.
Research Protocol No. 309 has been approved on September 19th, 2017 by the Local Ethical Committee in accordance with the ethical principles of scientific research provided by the World Medical Association in the Declaration of Helsinki.
The study included questionnaires, anthropometry (measurement of height, weight, waist circumference (WC), calculation of body mass index (BMI), measurement of blood pressure (BP), determination of biochemical parameters: glycated hemoglobin (HbA1c,%), C-peptide, Insulin, fasting capillary blood glucose, lipid profile: low density lipoprotein (LDL), high density lipoprotein (HDL), triglycerides, total cholesterol, Endocan and PAI-1 biomarkers, IR-HOMA index was calculated.
The survey included questions of socio-demographic characteristics, heredity, history of chronic non- infectious diseases, and drug intake.
Blood pressure (BP) was measured in accordance with the WHO guidelines using a mechanical tonometer (Microlife BP AG1–10) on both arms with a preliminary rest period of at least 10 minutes. The smallest of three consecutive measurements was taken for calculations.
Height and weight were measured using a digital weighted stadiometer (TBEC RS-232). Body mass index (BMI) was calculated using the formula: body weight divided by the square of height in meters (kg/m2). Waist circumference (WC, cm) was measured using an inelastic measuring tape at the midpoint between the lower edge of the last palpable rib and the top of the iliac crest. BMI was graded according to “Centers for Disease Control and Prevention”: from 25.0 to 30.0 kg/m2 as overweight, more than 30.0 kg/m2 as various degrees of obesity. Abdominal obesity was considered if WC was over 94 cm in males, and over 88 cm in females.
Measurement of biochemical parameters.
The plasma with Ethylenediaminetetraacetic acid (EDTA) was conserved in vials by aliquots and quickly frozen. The samples were stored at -70 degrees Celsius for no more than 3 months. Determination of fasting lipid profile blood test (Total cholesterol LDL, HDL, triglycerides) was done from blood plasma by the method of selective precipitation with phosphotungstate and magnesium. HbA1c was determined from capillary whole blood by reflectometry using the Nyco-Card test system. Determination of insulin, glucagon, C-peptide was carried out by multiplex immunological analysis using xMap technology on Bioplex 3D.
Measurement of endothelial dysfunction biomarkers: Endocan, PAI-1.
The method of magnetic bead-based multiplex immunoassay using xMap technology was used for Endocan and PAI-1. The standard Milliplex map Human Cardiovascular Disease Magnetic Bead Panel 1 (Millipore) kit was used to determine concentration of listed metabolites in accordance with “Override protocol” instruction of manufacturer. The study protocol included incubation of unknown, standard, and control samples with magnetic beads loaded with primary antibodies, revelation using detecting antibodies and Streptavidin Phycoerythrin Conjugated. Final step of the protocol was fluorescence registration using Bioplex 3D equipment (Luminex software). The coefficient of variation was less than 20 % for all detected analytes with minimum detectable concentration of Endocan — 430.55 pg/ml, PAI-1 — 3489.3 pg/ml.
Measurement of Intima Media Thickness
Carotid artery IMT measurement was performed by one well-trained, certified specialist. IMT of the carotid artery was defined as the average result of measuring the thickness of tunica intima media of the right and left common carotid artery (CCA), which was visualized as a double-line sign longitudinally CCA.
Ultrasound studies were carried out, in B-mode, real-time ultrasonography using the Philips EPIQ 7 equipment.
According to the ESC / ESH guideline, the ultrasound value of carotid IMT is more than 0.9 mm, the maximum of the two values (right and left) was considered the presence of an atherosclerosis [11]. In addition, the visualization of the plaques themselves was considered also as an atherosclerosis. Carotid plaque was defined as focal extrusion into the lumen of the artery by at least 0.5 mm or 50 % of the surrounding IMT of the carotid artery, or> 1.5 mm thick.
Assessment of cardiovascular risk using the SCORE scale.
The SCORE scale allows assessing the ten-year risk of developing CVE and mortality from them. Risk calculation was carried out using an online calculator, as well as using risk scales that are freely available [12].
Calculation of IR-HOMA index.
The IR-HOMA index was calculated using the formula (fasting insulin (μU/l) × fasting glucose (mmol/L) / 22.5), values greater than 2.7 were considered as IR.
Statistical analysis.
The data were tested for normal distribution using the Kolmogorov-Smirnov test. The distribution was abnormal. Variables with an abnormal distribution were transformed to normal distribution. The statistical significance of the differences between the groups (high / low diabetes risks) was assessed by the Student's t-test; the differences were considered statistically significant at p<0.05. Data were presented as Mean ± SD.
Evaluation of the relationship between the parameters of IMT, Endocan, PAI-1, biochemical, anthropometric parameters, blood pressure with the risk of diabetes, atherosclerosis, was carried out using correlation analysis. The Pearson's correlation coefficient was used (IMT, PAI-1, LDL, HDL, fasting glycemia, Diastolic BP) for data with a normal distribution. As for abnormal distribution, the Spearman's correlation coefficient was used (BMI, WC, Systolic BP, IR-HOMA index, SCORE, C-peptide, Insulin, total cholesterol, triglycerides).
Binary logistic regression analysis was done to assess the factors affecting the IMT, dependent variable was the presence/absence of atherosclerosis, the adjustment was done by gender, age, and the presence of arterial hypertension. The results were considered statistically significant at p<0.05.
Statistical analysis was performed using IBM SPSS Statistics, 22.0.
Results
Table 1 presents the characteristics of the respondents.
Table 1
Characteristics of respondents with various risks of type 2 diabetes
|
Variables |
Low risk of T2DM, n = 138 |
High risk of T2DM, n = 46 |
p-level |
|
Age, years |
45.11±12.59* |
54.62±9.97 |
0.07 |
|
BMI, kg/m2 |
26.37±5.02 |
32.37±5.41 |
0.03 |
|
WC, cm |
88.03±14.21 |
104.27±12.52 |
0.02 |
|
Systolic BP, mm of mercury |
117.3±18.9 |
131.6±15.2 |
0.05 |
|
Diastolic BP, mm of mercury |
76.8±11.6 |
83.32±10.4 |
0.06 |
|
Fasting glucose, mmol/l |
5.59±0.7 |
5.86±0.9 |
0.05 |
|
HbA1c,% |
5.59±0.74 |
5.76±0.32 |
0.05 |
|
Insulin, mU/l |
8.95±10.7 |
13.97±15.02 |
0.05 |
|
IR-HOMA index |
2.44±3.8 |
3.88±4.8 |
0.05 |
|
C-peptide, pg/ml |
1334.07±2894.2 |
1506.9±899.7 |
0.05 |
|
Total cholesterol, mmol/l |
5.85±1.98 |
5.92±1.65 |
0.07 |
|
LDL, mmol/l |
3.72±1.07 |
4.0±1.04 |
0.08 |
|
HDL, mmol/l |
1.20±0.40 |
1.13±0.5 |
0.06 |
|
Triglycerides, mmol/l |
1.22±1.04 |
1.28±0.81 |
0.07 |
|
SCORE, % |
2.5±2.84 |
3.35±0.99 |
0.01 |
|
PAI-1, pg/ml |
29042.13±17490.91 |
32307.15±19947.12 |
0.05 |
|
Endocan, pg/ml |
803.7±143.2 |
1698.2±576.2 |
0.01 |
|
Right CCA IMT, mm |
0.74±0.22 |
0.90±0.15 |
0.05 |
|
Left CCA IMT, mm |
0.75±0.16 |
0.91±0.14 |
0.02 |
|
*Data are presented as Mean±SD |
Differences between the groups were found, so BMI and WC predictably prevailed in the group with a high risk of type 2 diabetes. It reflected the presence of obesity 1 degree; BMI-32.37±5.41 kg/m2, p = 0.03, abdominal obesity; WC-104.27 ± 12.52 cm; p = 0.02 compared to group of low diabetes risk.
Systolic BP predominated in the group with a high risk of T2DM, and reflected in this group the presence of arterial hypertension of 1 degree, according to the American Heart Association guidelines.
The predominance insulin resistance indicators and carbohydrate metabolism, what included fasting glycemia, glycated hemoglobin, insulin, C-peptide, and the IR-HOMA index was also established in patients with a high risk of T2DM.
There no differences were found in the groups in the study of lipid metabolism (lipidogram). However, dyslipidemia occurred in both groups, more pronounced in the group of patients with high diabetes risk.
Cardiovascular risk (CVR) according to the SCORE scale was also higher in the group of patients with a high risk of T2DM 3.35 ± 0.99 %; (p = 0.01), and reflected a moderate CVR (23.24).
Concentrations of the biomarkers Endocan and PAI-1 prevailed in the group with a high risk T2DM and amounted to 1698.2±576.2; p = 0.01 and 32307.15±19947.12 pg/ml; p = 0.05 respectively.
Ultrasound examination of CCA IMT revealed the following differences. The prevalence of CCA IMT of the left was established in patients in the group of high diabetes risk, compared with group of low diabetes risk. Thus, CCA IMT of the right was 0.90±0.15; p = 0,05 mm; CCA IMT of the left was 0.91±0.14 mm; p = 0.02 and reflected the presence of subclinical atherosclerosis.
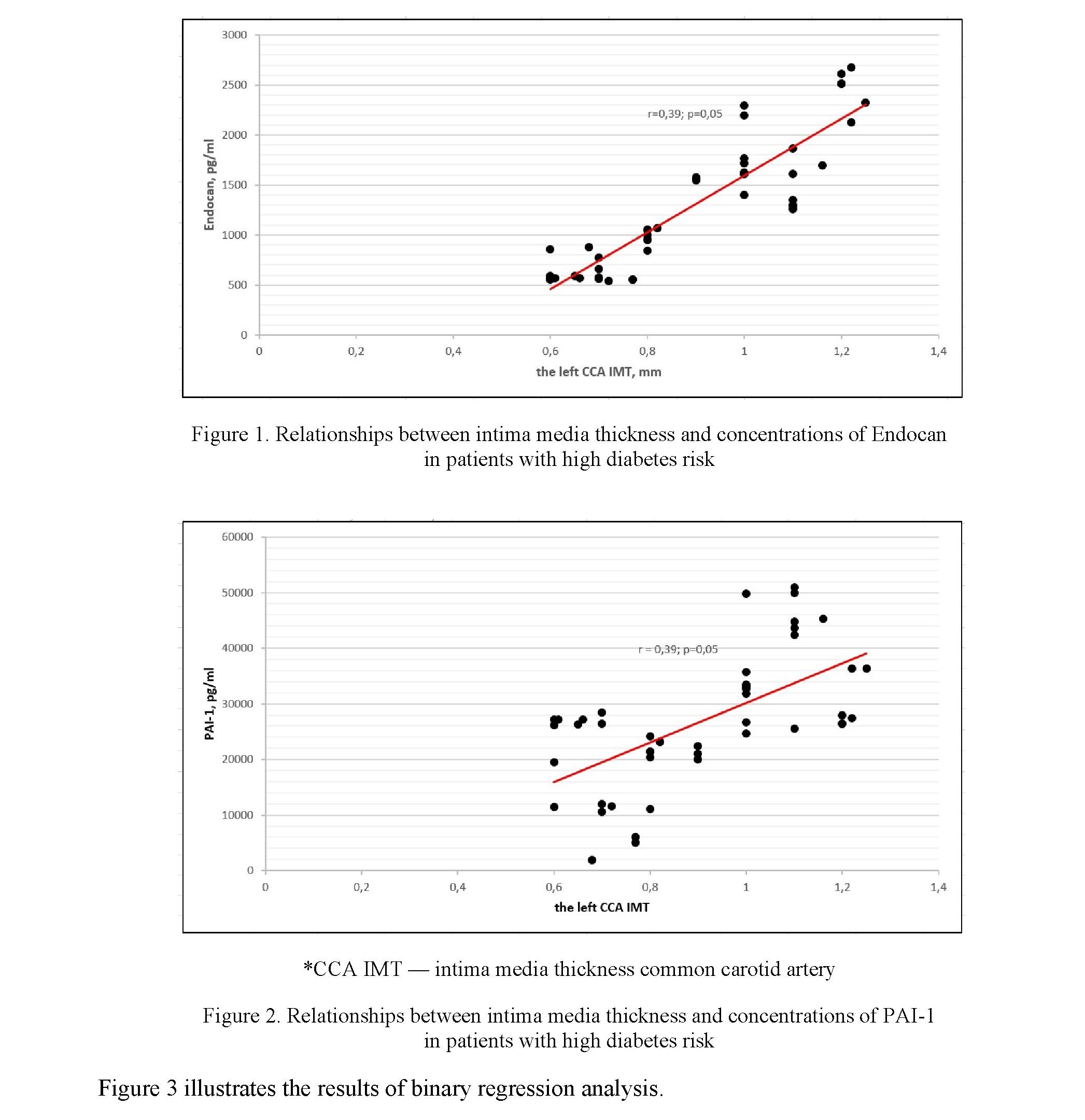
Correlation analysis of factors affecting intima media thickness (subclinical atherosclerosis), Endocan and PAI-1 levels in patients with a high risk of T2DM are presented in Table 2, Figures 1 and 2.
The increase of CCA IMT, in addition to well-known indicators such as (BMI, WC, Systolic BP, Diastolic BP, total cholesterol, HDL, triglycerides), was found to be influenced by an increase in FINDRISC scores (r = 0.41; p = 0.05), on the SCORE scale (r = 0.69; p = 0.001), fasting glycemia (r = 0.98; p = 0.001), increased glycated hemoglobin (r = 0.49; p = 0.02), insulin (r = 0.36; p = 0.03), IR-HOMA (r = 0.47; p = 0.05), Endocan (r = 0.86; p ≤ 0.001), and PAI-1 level (r = 0.39; p = 0.05), (Fig. 1 and 2).
Correlation analysis has established factors affecting the increase in the Endocan and PAI-1 level, (Table 2). To increase both biomarkers of endothelial dysfunction affect increasing scores on FINDRISC scale, an increase in BMI and WC, hyperglycemia, hyperinsulinemia, increasing IR-HOMA index, increasing concentrations of С-peptide and LDL. A subclinical atherosclerosis development is affected by an increase in the level of Endocan (r = 0.85; p = ≤0.001), (Fig. 1) and PAI-1 (r = 0.39; p = 0.01), (Fig. 2). Moreover, the correlations of IMT are stronger with the biomarker Endocan. Both biomarkers lead to increasing cardiovascular risk in the SCORE scale.
Table 2
Correlation analysis of factors affecting the intima media thickness (subclinical atherosclerosis), the level of Endocan and PAI-1 in patients with a high risk of T2DM, (r)
|
Variables |
*IMT>0.9 mm (ath: yes/no) |
p-level |
Endocan |
p-level |
PAI-1 |
p-level |
|
r |
r |
r |
||||
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
FINDRISC (high/low risk T2DM) |
0.41 |
0.05 |
0.51 |
≤0.001 |
0.31 |
0.05 |
|
BMI, kg/m2 |
0.21 |
0.05 |
0.27 |
0.04 |
0.22 |
0.02 |
|
WC, cm |
0.27 |
0.02 |
0.32 |
0.03 |
0.33 |
0.03 |
|
Systolic BP, mm of mercury |
0.88 |
0.004 |
0.36 |
0.03 |
0.09 |
0.1 |
|
Diastolic BP, mm of mercury |
0.68 |
0.05 |
0.08 |
0.1 |
0.04 |
0.5 |
|
HbA1c, % |
0.49 |
0.02 |
0.23 |
0.04 |
0.36 |
0.02 |
|
Fasting glucose, mmol/l |
0.98 |
≤0.001 |
0.22 |
0.02 |
0.24 |
0.002 |
|
Insulin, μU/l |
0.36 |
0.03 |
0.27 |
0.02 |
0.41 |
0.008 |
|
IR-HOMA index |
0.47 |
0.05 |
0.37 |
0.01 |
0.47 |
0.003 |
|
C-peptide, pg/ml |
0.17 |
0.04 |
0.23 |
0.02 |
0.39 |
0.01 |
|
Total cholesterol, mmol/l |
0.36 |
0.05 |
0.07 |
0.5 |
0.05 |
0.9 |
|
LDL, mmol/l |
0.54 |
0.04 |
0.37 |
0.03 |
0.27 |
0.01 |
|
HDL, mmol/l |
–0.05 |
0.8 |
0.06 |
0.3 |
–0.03 |
0.7 |
|
Triglycerides, mmol/l |
0.41 |
0.03 |
0.27 |
0.03 |
0.05 |
0.4 |
|
SCORE,% |
0.69 |
0.001 |
0.57 |
≤0.001 |
0.45 |
0.05 |
|
Right CCAIMT, mm |
- |
- |
0.62 |
≤0.001 |
0.23 |
0.05 |
Continuation of Table 2
|
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
Left CCA IMT, mm |
- |
- |
0.85 |
≤0.001 |
0.39 |
0.05 |
|
Ath., (yes/no) |
- |
- |
0.85 |
≤0.001 |
0.39 |
0.01 |
|
PAI-1, pg/ml |
0.39 |
0.05 |
- |
- |
- |
- |
|
Endocan, pg/ml |
0.85 |
≤0.001 |
- |
- |
- |
- |
|
*Ath. — atherosclerosis, BMI — body mass index; WC — waist circumference; BP — blood pressure; HOMA — IR: homeostasis model for insulin resistance; LDL — low density lipoproteins; HDL — high density lipoprotein; SCORE: cardiovascular risk; CCA IMT — common carotid artery intima media thickness |
||||||
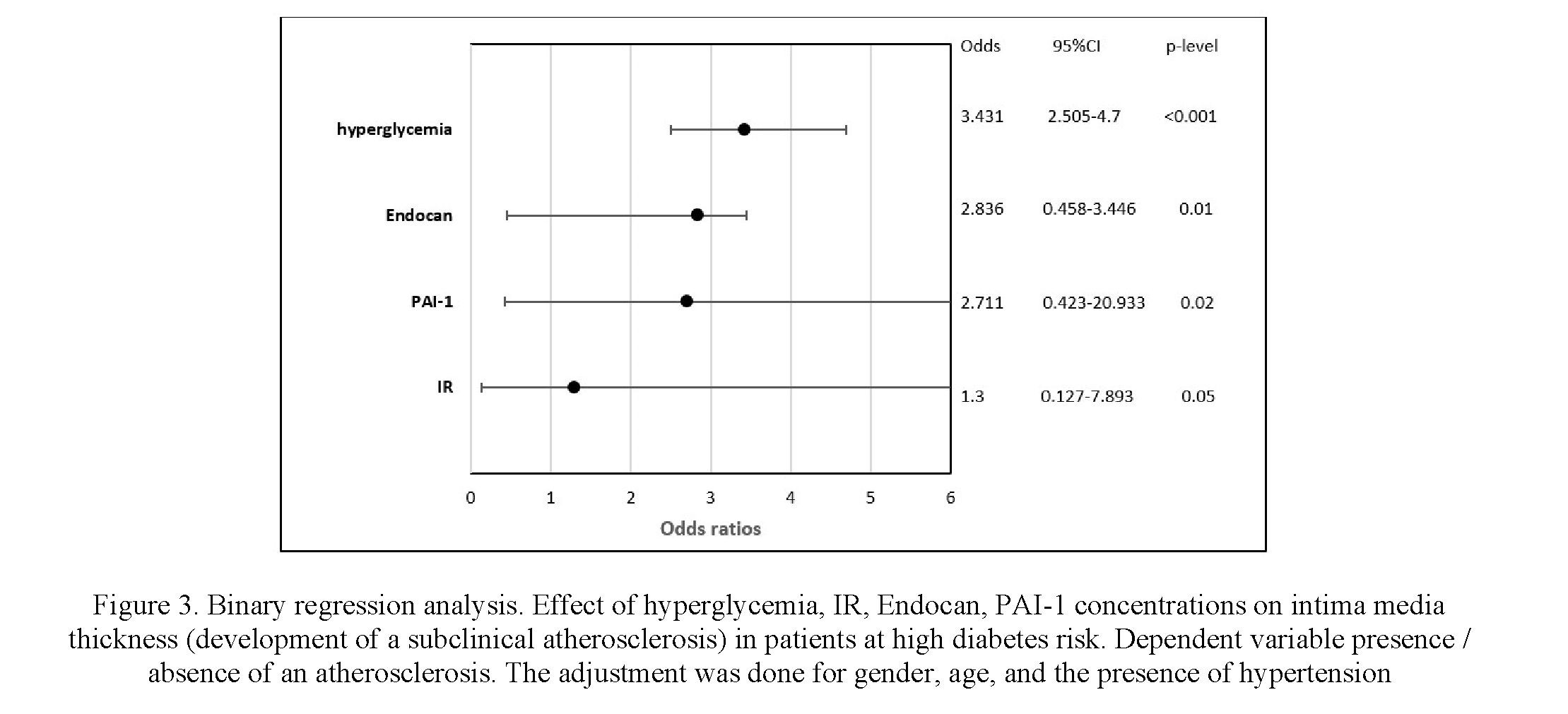
Binary regression analysis with correction for sex, age, and the presence of hypertension has revealed the following. Hyperglycemia by 3.4-fold (p<0.001) elevation concentrations of Endocan by 2.8-fold (p=0.01), and elevation of PAI-1 by 2.9-fold (p=0.02), Insulin resistance by 1.3-fold (p=0.05) affect the risk of development of a subclinical atherosclerosis. The results are presented as the Odd Ratio (OR). 95 % of confidence is interval for each OR.
Discussions
The results of our study showed that patients with high diabetes risk have a high CVR due to the presence of insulin resistance, subclinical atherosclerosis, as well as the presence of endothelial dysfunction, which is simultaneously confirmed by high levels of the Endocan and PAI-1 biomarkers and their effect on IMT in patients of the studied group.
Assessment of the endothelial dysfunction biomarkers such as Endocan and PAI-1 in patients at risk of T2DM using the FINDRISC scale has not been performed. Moreover, the simultaneous assessment of the Ratio of IMT and levels of Endocan, PAI-1 biomarkers in patients with diabetes risk has also not been studied previously.
Biomarker — Plasminogen activator inhibitor-1 (PAI-1) is a vascular factor [13], a fast-acting inhibitor of fibrinolysis, is considered as one of the risk factors triggering atherosclerosis [14] and, as a result, the risk of CHD. Endocan is an early biomarker of ED, which is influenced by insulin resistance, various disorders of carbohydrate metabolism, including hyperglycemia and impaired glucose tolerance [15].
PAI-1 biomarker is considered a predictor of T2DM. According to the study [16], the PAI-1 biomarker predicted the development of T2DM, regardless of IR and other known risk factors (body mass index, waist circumference, gender, age). Diabetes developed in 140 (16.6 %) of 843 people after a 5-year follow-up period [16]. The question whether the endothelial dysfunction affects the increase in diabetes is not fully clarified examined despite many scientists studied Endocan only in patients with the verified T2DM [17–19].
There is a single study examining IMT in patients at risk of T2DM [10]. In the study, Kiss et al. found an increased chance of developing subclinical atherosclerosis in patients at high risk T2DM. These findings are also consistent with the results of our study.
The effect of PAI-1 level on IMT was studied in separate studies in patients without carbohydrate metabolic disorders. Thus, a study by Marchesi et al. [20] established the effect of PAI-1 on IMT in patients with hypertension. Carratala et al. [21] established the effect of PAI-1 on IMT in patients with hyperlipidemia. Also, Endocan has been studied in patients without impaired carbohydrate metabolism; in CVD, such as ischemic heart disease, [22, 23] acute myocardial infarction [24–26], and arterial hypertension [27]. Our study reveled the relationship between the levels of PAI-1, Endocan, and IMT CCA, the impact of carbohydrate metabolism disorders, IR on the development of ED, and as a result, the development of subclinical atherosclerosis.
Furthermore, as the PAI-1 biomarker is a vascular factor [28], one of the risk factors triggering atherosclerosis [14], PAI-1 is produced by various cells of adipose tissue, including preadipocyte, mature adipocytes, macrophages, endothelial, and smooth muscle cells [29].
Besides, hyperglycemia can affect the PAI-1 level. Maiello et al. [30] identified that high glucose level reduced the fibrinolytic capacity of endothelial cells. In an experimental study on rats, Chen et al. [31] demonstrated that hyperglycemia stimulated the activation of the PAI-1 gene promoter in vascular smooth muscle cells.
There is no study on the assessment of the relationships between the Endocan biomarker level and CCA IMT in patients with diabetes risk or prediabetes. However, there are similar studies on patients with T2DM, with varying degrees of compensation for hyperglycaemia [15, 18], where the level Endocan was increased. Thus, a positive association was determined between the level of Endocan and IMT, respectively, and subclinical atherosclerosis in patients with T2DM [19]. Probably, the high level of Endocan was a result of the accomplished endothelial dysfunction in this category of patients with T2DM. Pathogenetic mechanisms of the relationship between the Endocan biomarker and impaired carbohydrate metabolism in patients not only with prediabetes but also with T2DM are still not fully understood. Thus, the main question as follows: Is the elevation of Endocan in patients with T2DM evidence of angiopathy, or a manifestation of incipient endothelial dysfunction, aggravated by impaired carbohydrate metabolism (hyperglycemia)?
In our study, we obtained correlations between the Endocan, PAI-1 level, and blood glucose, IR indicators. This also highlights the contribution of impaired carbohydrate metabolism to the development of ED in patients with high diabetes risk.
The study [32] revealed the simultaneous presence of IR and worsening insulin sensitivity in patients with ED and without diabetes. PAI-1 levels were higher in patients with ED [33]. In our study, the PAI-1 level was higher in the group of patients with a high risk of T2DM and increased the likelihood of development subclinical atherosclerosis in this category of patients by 2.9-fold. This determines the importance of studying this marker at the stage of diabetes risk or earlier to prevent the development of both T2DM and cardiovascular events, and targeting the factors that affect the increase in this biomarker.
Further monitoring of the identified high-risk group of T2DM is necessary to track the development of both T2DM and vascular events, and future changes of concentrations Endocan and PAI-1. It is necessary to conduct further prospective observation of the study participants to assess the development of ED, T2DM, and cardiovascular events in the studied group.
Conclusions
The presence of IR and disorders of carbohydrate metabolism was found in patients with a high risk of T2DM. Endothelial dysfunction was established in the form of a subclinical atherosclerosis and an increase of Endocan, PAI-1 concentration, in this study group of high risk of T2DM.
An elevation of biomarkers endothelial dysfunction, Endocan and PAI-1 increases the likelihood of the development of a subclinical atherosclerosis in patients with a high diabetes risk.
The high levels of Endocan and PAI-1 biomarkers in those examined with a high diabetes risk determines the importance of planning a clinical strategy for the timely identification of this category of patients and conducting targeted therapeutic interventions, which will prevent both the development of T2DM and endothelial dysfunction, and reduce further cardiovascular risk.
Acknowledgements
This study was funded by the Ministry of Health of the Republic of Kazakhstan under the scientific and technical program О.0769 “Development of the scientific basis for the formation of a preventive environment in order to preserve public health”.
References
- Kannel, W.B., & McGee, D.L. (1979). Diabetes and cardiovascular risk factors: the Framingham study. Circulation, 59; 8. https://doi.org/10.1161/01.CIR.59.1.8
- World Health Organization (2021). Cardiovascular diseases (CVDs). Retrieved from https://www.who.int/news-room/fact- sheets/detail/cardiovascular-diseases-(cvds)
- World Health Organization (2018). Health of the Population of the Republic of Kazakhstan and the Activities of Health Organizations in 2017. Astana, Kazakhstan.
- Janus, A., Szahidewicz-Krupska, E, Mazur, G., & Doroszko, A. (2016). Insulin Resistance and Endothelial Dysfunction Constitute a Common Therapeutic Target in Cardiometabolic Disorders. Mediators of Inflammation, 2016. https://doi.org/10.1155/2016/3634948
- Alssema, M., Feskens, E.J., Bakker, S.J., Gansevoort, R.T., Boer, J.M., Heine, R.J., Nijpels, G., Stehouwer, C.D., van der Kraan, M., & Dekker, J.M. (2008). Finnish questionnaire reasonably good predictor of the incidence of diabetes in The Netherlands. Ned Tijdschr Geneeskd., 1–152 (44); 2418–2424.
- López-González, Á.A., García-Agudo, S., Tomás-Salvá, M., Vicente-Herrero, M.T., Queimadelos-Carmona, M., & Campos- González, I. (2017). FINDRISC Test: Relationship between cardiovascular risk parameters and scales in Spanish Mediterranean population. Rev Med Inst Mex Seguro Soc., 55 (3); 309–316.
- Mamedov, M.N., Korneeva, V.N., & Oynotkinova, O.S. (2017). Assessment of Relationship between Cardiovascular Risk and Risk of Development of Diabetes Mellitus. Kardiologiia, 57(2); 46–51.
- Fizelova, M., Jauhiainen, R., Stančáková, A., Kuusisto, J., & Laakso, M. (2016). Finnish Diabetes Risk Score Is Associated with Impaired Insulin Secretion and Insulin Sensitivity, Drug-Treated Hypertension and Cardiovascular Disease: A Follow-Up Study of the METSIM Cohort. PLoS ONE, 16 (11); 11. https://doi.org/10.1371/journal.pone.0166584
- Laryushina, Y., Parakhina, V., Turmukhambetova, A., Turgunova, L., Ibraeva, L., Amirkhanova, D., & Nildibayeva, F. (2020). The Relationship Between the Level Fabp4, Risks of Type 2 Diabetes Mellitus, and Cardiovascular Events. Open Access Macedonian Journal of Medical Sciences, 10; 8(B); 762–768. https://doi.org/10.3889/oamjms.2020.4678
- Kiss, L.Z., Bagyura, Z., Vadas, R., Polgár, L., Lux, Á., & Édes, E. (2017). Signs of subclinical atherosclerosis in asymptomatic patients at increased risk of type 2 diabetes mellitus. J Diabetes Complications, 31 (8); 1293–1298. https://doi.org/10.1016/j.jdiacomp.2017.05.007
- Simova, I. (2015). Intima-media thickness: appropriate evaluation and proper measurement. The e-Journal of Cardiology Practice, 13; 21.
- Piepoli, F.M., Hoes, W.A., Agewsll, S., Albus, C., Brotons, C., Catapano L.A., Cooney, M.-T., Corra, U., Cosyns, B., Deaton, C., Graham, I., Hall., M.S., et al. (2016). European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice, Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). European Heart Journal, 37 (29); 2315–2381. https://doi.org/10.1093/eurheartj/ehw106
- Adly, A.A., Elbarbary, N.S., Ismailm E.A., & Hassan, S.R. (2014). Plasminogen activator inhibitor-1 (PAI-1) in children and adolescents with type 1 diabetes mellitus: relation to diabetic micro-vascular complications and carotid intima media thickness. J Diabetes Complications, 28(3); 340–347. https://doi.org/10.1016/j.jdiacomp.2014.01.011
- Tretjakovs, P., Jurka, A., Bormane, I., Mikelsone, I., Elksne, K., & Krievina, G. (2012). Circulating adhesion molecules, matrix metalloproteinase-9, plasminogen activator inhibitor-1, and myeloperoxidase in coronary artery disease patients with stable and unstable angina. Clinica Chimica Acta, 413; 25–29. https://doi.org/10.1016/j.cca.2011.10.009
- Balamir, I., Ates, I., Topcuoglu, C., & Turhan, T. (2018). Association of Endocan, Ischemia-Modified Albumin, and hsCRP Levels With Endothelial Dysfunction in Type 2 Diabetes Mellitus. Angiology, 69 (7); 609–616.https://doi.org/10.1177/0003319717740781
- Festa, A., D'Agostino, R. Jr., Tracy, R.P., & Haffner, S.M. (2002). Elevated levels of acute-phase proteins and plasminogen activator inhibitor-1 predict the development of type 2 diabetes: the insulin resistance atherosclerosis study. Diabetes, 51 (4); 1131– 1137. https://doi.org/10.2337/diabetes.51.4.1131.
- Festa, A., Williams, K., Tracy, R.P., Wagenknecht, L.E., & Haffner, S.M. (2006). Progression of plasminogen activator inhibitor-1 and fibrinogen levels in relation to incident type 2 diabetes. Circulation, 113(14); 1753–1759. https://doi.org/10.1161/CIRCULATIONAHA.106.616177
- Dallio, M., Masarone, M., Caprio, G., Sarno, R., Tuccillo, C., & Sasso, F.C. (2017). Endocan Serum Levels in Patients with Non-Alcoholic Fatty Liver Disease with or without Type 2 Diabetes Mellitus: A Pilot Study. J Gastrointestin Liver Dis., 26 (3); 261– 268. https://doi.org/10.15403/JGLD.2014.1121.263.DAL
- Lv, Y., Zhang, Y., & Shi, W. (2017). The Association Between Endocan Levels and Subclinical Atherosclerosis in Patients With Type 2 Diabetes Mellitus. Am J Med Sci., 353(5); 433–438. https://doi.org/10.1016/j.amjms.2017.02.004
- Marchesi, E., Martignoni, A., Tinelli, C., Ravetta, V., Resasco, T., & Piredda, M. (1999). Plasminogen activator inhibitor-1 and carotid intima-media thickening in patients with newly detected primary hypertension. J Cardiovasc Risk., 6(6); 363– 369. https://doi.org/10.1177/204748739900600602
- Carratala, A., Martinez-Hervas, S., Rodriguez-Borja, E., Benito, E., Real, J.T., & Saez, G.T. (2018). PAI-1 levels are related to insulin resistance and carotid atherosclerosis in subjects with familial combined hyperlipidemia. J Investig Med., 66(1); 17–21. http://dx.doi.org/10.1136/jim-2017-000468
- Kundi, H., Gok, M., Kiziltunc, E., Topcuoglu, C., Cetin, M., & Cicekcioglu, H. (2017). The Relationship Between Serum Endocan Levels With the Presence of Slow Coronary Flow: A Cross-Sectional Study. Clin Appl Thromb Hemost., 23(5); 472–477. https://doi.org/10.1177/1076029615618024
- Ye, M.F., Zhao, Z.W., Luo, Y.K., Dong, X.F., & Yan, Y.M. (2016). Elevated endocan concentration is associated with coronary slow flow. Scand J Clin Lab Invest., 76(5); 345–348. https://doi.org/10.1080/00365513.2016.1177853.
- Kundi, H., Balun, A., Cicekcioglu, H., Karayigit, O., Topcuoglu, C., & Kilinckaya, M.F. (2017). Admission Endocan Level may be a Useful Predictor for In-Hospital Mortality and Coronary Severity Index in Patients With ST-Segment Elevation Myocardial Infarction. Angiology, 68 (1); 46–51. https://doi.org/10.1177/0003319716646932
- Qiu, C.R., Fu, Q., Sui, J., Zhang, Q., Wei, P., & Wu, Y. (2017). Serum Endothelial Cell-Specific Molecule 1 (Endocan) Levels in Patients With Acute Myocardial Infarction and Its Clinical Significance. Angiology, 68(4); 354–359. https://doi.org/10.1177/0003319716651349
- Qiu, C.R., Fum Q,, Sui, J., Zhang, Q., Wei, P., & Wu, Y. (2017). Analysis of Serum Endothelial Cell-Specific Molecule 1 (Endocan) Level in Type 2 Diabetes Mellitus With Acute ST-Segment Elevation Myocardial Infarction and its Correlation: A Pilot Study. Angiology, 68(1); 74–78. https://doi.org/10.1177/0003319716634581
- Balta, S., Mikhailidis, D.P., Demirkol, S., Ozturk, C., Kurtoglu, E., & Demir, M. (2014). Endocan-a novel inflammatory indicator in newly diagnosed patients with hypertension: a pilot study. Angiology, 65(9); 773–777.https://doi.org/10.1177/0003319713513492
- Adly, A.A., Elbarbary, N.S., Ismail, E.A., & Hassan, S.R. (2014). Plasminogen activator inhibitor-1 (PAI-1) in children and adolescents with type 1 diabetes mellitus: relation to diabetic micro-vascular complications and carotid intima media thickness. J Diabetes Complications, 28(3); 340–347. https://doi.org/10.1016/j.jdiacomp.2014.01.011
- Bastelica, D., Morange, P., & Berthet, B. (2002). Stromal cells are the main plasminogen activator inhibitor-1-producing cells in human fat: evidence of differences between visceral and subcutaneous deposits. Arteriosclerosis, Thrombosis, and Vascular Biology, 22; 173–178. https://doi.org/10.1161/hq0102.101552
- Maiello, M., Boeri, D., Podesta, F., Cagliero, E., Vichi, M., & Odetti, P. (1992). Increased expression of tissue plasminogen activator and its inhibitor and reduced fibrinolytic potential of human endothelial cells cultured in elevated glucose. Diabetes, 41; 1009–1015. https://doi.org/10.2337/diab.41.8.1009
- Chen, Y.-Q., Sum M., Raja Walia, R., Hao, Q., Cowington, J.W., & Vaughan, D.E. (1998). Sp1 sites mediate activation of the plasminogen activator inhibitor-1 promoter by glucose in vascular smooth muscle cells. J Biol Chem., 273; 8225–8231. https://doi.org/10.1074/jbc.273.14.8225
- Lalić, K., Nedeljković, M., Jotić, A., Babić, R., Rajković, N., & Popović, L. (2018). Endothelial dysfunction of coronary arteries in subjects without diabetes: an association with both insulin resistance and impaired insulin secretion response. Diabetes Res Clin Pract., 139; 179–187. https://doi.org/10.1016/j.diabres.2018.03.005
- Erzen, B., & Sabovic, M. (2013). In young post-myocardial infarction male patients elevated plasminogen activator inhibitor- 1 correlates with insulin resistance and endothelial dysfunction. Heart Vessels, 28; 570–577. https://doi.org/10.1007/s00380-012- 0287-9